
What is a full tongue-tie release? Hint: It’s not a clip or a snip!
I don’t like the term “clip” or “snip.” Those are four-letter words to me. If I hear a baby or child was clipped or snipped, about 95% of the time it wasn’t enough.
Normally a clip or snip is performed by a provider at the hospital or in the office (ENT or pediatrician), or while the child was put to sleep (it’s not necessary to put kids to sleep for this procedure, but that’s another topic).
Warning images of tongues ahead…
The proper term is really a release of the tight tissue, so providers who are up-to-date will call the procedure a “release” instead of clip or snip. The concept that treating a tongue-tie is “no big deal” is what leads to the problem with the clip. If they do a clip, they will almost always cut halfway with scissors, and leave a thick band of tissue.
If it’s cut halfway, it will work half the time.
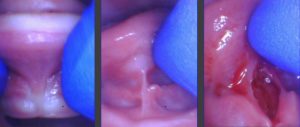
They think they are getting it all, but in reality, if you were to lift up on the tongue, it ends up looking like this:

See that thick band of tissue left behind? That’s going to limit mobility and function- and it’s not going to have nearly the success rate.
When we use our technique to get a full release, every time, we get a nice diamond-shaped wound that allows for the full lift of the tongue with minimal to no bleeding.
 The physicians performing this procedure are great at other aspects of medicine and are well-meaning… but the clips we see and have to properly release on a daily basis are inadequate and sometimes even damaging to parts of the tongue and floor of the mouth.
The physicians performing this procedure are great at other aspects of medicine and are well-meaning… but the clips we see and have to properly release on a daily basis are inadequate and sometimes even damaging to parts of the tongue and floor of the mouth.
The baby below was cut into the body of the tongue (see the white area above the string), and we released it properly and saw a great improvement in symptoms. The restrictive lip-tie was also not seen, or not deemed to be a problem.
This baby was clipped at the hospital by the pediatrician and her salivary gland openings were turned into a cluster of grape-like openings because the provider clipped right through them and missed the string. Here’s the proper release on that same patient after we used the CO2 laser. Notice the better elevation of the tongue. 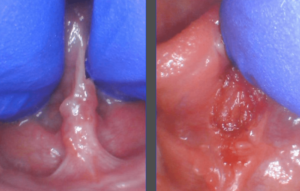
The increased mobility in a clip or snip is enough for some kids or babies to now compensate, but many kids and babies will still struggle, and moms will continue to have symptoms.
It’s just effective enough to reduce nipple pain and help with speech a little bit, so that’s one reason why the research on tongue-ties has been muddied for a season. Most studies on tongue-ties are done with incomplete clips or snips.
It’s just effective enough for providers to think they are offering a great service to patients when in reality, many of them continue to struggle or see a return of symptoms.
Why is this being done?
The reason for the halfway clip is to avoid the vascular region under the tongue because a misplaced clip can cause significant bleeding and complications.
It’s also being done that way because that’s how medical schools and residencies are training the doctors to do them. We received no formal training in dental school or residency as a pediatric dentist… so there is a huge lack of education in our current system.
 When providers do learn how to clip, it’s a watch one – do one – teach one method. The senior doctor says – “Oh here’s a tongue-tie, it’s easy. Just snip here and you’re done.” Then the resident goes and does one. Then he or she teaches another how to do it. And misinformation spreads and is perpetuated by anecdotal evidence and a mentality that tongue-ties rarely cause problems and they are simple to manage.
When providers do learn how to clip, it’s a watch one – do one – teach one method. The senior doctor says – “Oh here’s a tongue-tie, it’s easy. Just snip here and you’re done.” Then the resident goes and does one. Then he or she teaches another how to do it. And misinformation spreads and is perpetuated by anecdotal evidence and a mentality that tongue-ties rarely cause problems and they are simple to manage.
In reality, it requires a team approach to manage, a full assessment and history of symptoms are critical, a proper release is needed, and follow-up exercises are necessary to prevent the two sides from growing back together.
What’s the difference?
Often these procedures are done without magnification loupes and good illumination and done from the front of the patient. Our method comes from behind the head, with the patient stabilized in a swaddle or with assistants holding for children, and uses 3.5x magnification with bright LED illumination so we can see the full restriction and provide the best possible treatment.
You cannot release what you cannot see.

Along those lines, when clipped or snipped with scissors, after the first cut, it immediately begins to bleed, hiding the rest of the thick fascia (connective tissue) underneath.
With the state-of-the-art CO2 laser, we are able to virtually paint over the area and it removes the tissue layer by layer with minimal to no bleeding, and we can release all the way because we can see it!
If your child had their tongue clipped or snipped and he or she is still struggling with feeding, speech, sleep, or you have a baby struggling with nursing or bottle-feeding issues, there is a good chance that it was done halfway.
Let us or have a knowledgable provider (up-to-date and has taken recent tongue-tie courses) take a look and get the rest of the tissue underneath to give the child the best chance of thriving and normal development.
A clipped or snipped tongue will persist and not stretch over time.
We see adults (like the one below) who have been clipped as a baby and still have a very tight attachment limiting their mobility and function. If a tongue cannot elevate close to the palate, the patient will have continued struggles.

Please get your baby or child released properly. Current struggles as well as future speech, feeding, and sleep as well as development depends upon a full and functional release. If you’re interested in our services, send us a message or call us at 205-419-4333.
If you’re a provider and would like to learn how to perform a full release, check out our online courses, or attend our live patient course after completing some of the online courses or live conferences.
A tongue-tie release is often life-changing for patients when done properly with a full assessment, proper technique, and good follow-up care.
Leave a comment if you have had experience with a clip or snip, or share with your friends so they can avoid this all-too-common outcome.