
If you read the news headlines, it sure sounds like it!
A recent article came out in the Journal of the American Medical Association (JAMA – ENT), which is a high impact journal. The article discussed looking into different reasons for feeding problems in infants, and still recommended many of them to have tongue-tie releases.
Unfortunately, the news media spun the article as “Babies ‘Don’t Need Tongue-Tie Surgery to Feed’” from the BBC. Others from Today, NYT, etc. all said virtually the same thing; babies don’t need their tongue’s clipped. I agree- they don’t need a clip, they need a full release, as discussed in a previous post.
But these people are actually arguing that we should leave a known physical barrier to normal development and life skills in children with diagnosed feeding problems. If there is a problem with feeding, the article suggested giving reflux medication, pushing them on the boob harder, tapping their feet or using a cold washcloth on the baby to wake it up… They are treating symptoms of tongue-tie problems instead of the ROOT cause – THE RESTRICTION!
If a child had webbed fingers, their fingers were fused together, no one would argue to leave them fused. Why? Because it’s obvious those will limit that child’s future and chances at normal growth and development.
He may not be a concert pianist or a pro athlete, but even just at a desk job or in school, he will need his fingers!

It’s so obvious it’s simple. If a tongue-tie is causing a problem, then release it. If it’s not causing a problem at the moment, counsel the parents it may cause a problem in the future, and let it be.
What’s really going on?
It seems that the increase in tongue-tie procedures has been worrying to the medical community, and they are concerned that babies and kids are getting their tongues clipped more than they were in the past.
In the past, if a baby had a feeding problem, they would say “Here’s a bottle. Good luck!” In the 1920s when formula came out, they told people that infant formula was better than breastmilk. They also told people that 9 out of 10 doctors smoked Camel! So clearly, we don’t need to fix the tongue-tie (as they had for hundreds of years) they would give them a bottle instead. Problem solved! 
Or so they thought… decades went by, and removing the tongue-tie surgically fell out of favor. Medical residencies and curricula stopped teaching that it was a problem. Or they said it “rarely causes issues.” They said a child will fall down and rip the lip-tie – so just leave it.
Hence, decades of undiagnosed tongue-ties built up – being in many cases a dominant gene, grandparents gave the condition to their kids, and they grew up and give it to their kids, so we are seeing more tongue-ties now than we used to see.
We are also more aware that tongue-ties that are further back from the tip (posterior) can also cause issues (starting in 2004, and really since 2014-2016). It doesn’t have to be to-the-tip to cause problems.
Any degree of restriction can cause any number of symptoms.
More and more providers and parents now realize hidden (posterior) tongue-ties can cause problems and we are diagnosing these at a higher rate.
Rates of tongue-tie are recorded in research at 4-10%, but this number does not include posterior tongue-ties. The number of babies and children with tongue-tie (or more appropriately a symptomatic tongue restriction) is probably closer to 20% (some would say more).
That’s 1 in 5 babies or children.
The epidemic is the most common reason for breastfeeding issues that cause moms to give up. It’s likely the most common cause of speech delay, speech problems, solid feeding issues, and sleep quality issues. In a typical classroom, the kid who finishes lunch last most likely has some type of tongue restriction. They will also have dark circles under their eyes and might have speech issues. If this describes your kid, please get him or her evaluated by a trained provider, or schedule a consult with us.
Just because something is being diagnosed more often, does not make it a “fad” as some claim. Is treating autism a fad because we are seeing it more often, and diagnosing it more?
That’s insulting to those suffering from the condition and shows that provider’s ignorance.
However, something more is happening.
We don’t know exactly why… some think it’s due to folic acid recommendations and MTHFR mutations that around half the population carries. Some think it could be all the pesticides, like RoundUp that are used on almost all of our crops in developed countries. It could be plastics, BPA (and similar compounds), flame retardants (in almost all upholstery). The amount of chemicals that we are exposed to before we are even born, is shocking. 287 were found in cord blood in one study!
Some compound, or recommendation, or practice (increased ultrasounds?) is happening in utero that is disturbing the tissue under the tongue from developing properly.
That is the headline that should be reported.
Instead, we focus on “Why are so many babies being treated?” Another answer to why they are being treated is BECAUSE IT WORKS! In almost every case, when done properly, it makes a difference in nursing, but also in speech, feeding, even sleep quality issues. With proper selection, therapy, technique, and aftercare, a patient can see life-changing results.
These life-changing stories are almost never reported by the media (here’s one where they did). It doesn’t serve their purposes. It doesn’t incite rage, anger, and get as many shares, likes, and comments on social media. Not to mention… the ones buying advertisements from the media companies control what is published. The formula industry is big business. Projected $62.5 BILLION dollars worldwide next year.
That’s a lot of money.
How much can corporations make off of a breastfed baby? Not much.
Not to mention, most infant formulas are made mostly of corn, soy, oil, and some type of hydrolyzed whey protein if it’s dairy-based. There are much better options, so please check the label if you choose to formula feed or supplement. This is NOT meant to guilt or mom shame, as we have many formula-fed babies we help who are struggling with bottle-feeding and tongue/lip-tie. (Just giving a bottle doesn’t solve the problem, and likely sets the child up for future issues.) However, these ingredients are cheap (subsidized even), easy to mass-produce and prioritize the profits of a company ahead of a baby’s health. Here’s a list of formula ingredients, and some healthier ones.
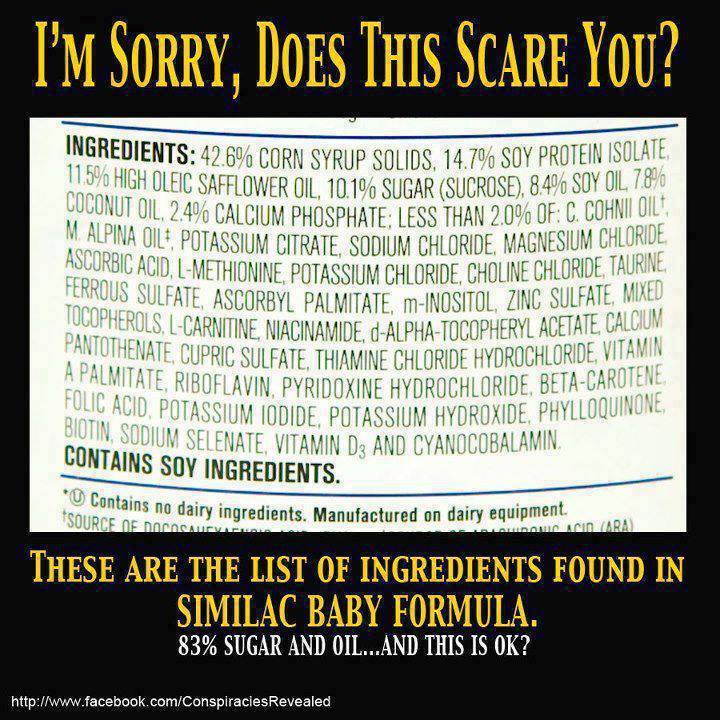
And 83% sugar. And we wonder why obesity is on the rise in America?
I was asked to participate in a Parent’s Magazine article about tongue-ties. They asked me, and I told them “Great! I’m so glad we can share the life-changing effects of tongue-tie treatment for kids.” Next email I heard back, they said “the editor has decided to go in a different direction for the piece. We no longer need you.” They jumped on the bandwagon of “tongue-ties don’t make a difference”. Just like the Atlantic did.
In response to the JAMA article that started the latest media blitz about tongue-ties a few weeks ago, my colleagues Soroush Zaghi, MD, Chelsea Pinto, DDS, and I decided to write a letter to the editor to advocate for the position that those in the tongue-tie professionals community take. That the procedure does make a big difference when done properly.
There were actually several issues with the methods the authors used. They even had the Kotlow tongue-tie grading scale backward. The article was only one author’s opinion but was being treated as an indisputable fact. They set out to try to reduce the number of procedures, and the babies didn’t have a proper follow-up.
Here is the letter to the editor we submitted to JAMA. This letter was balanced, well-edited, and respectful. It highlighted issues with the methods of the study without attacking the authors.
But it was rejected by the journal.
It was denied from being published or shared. Likely because they did not agree with our views.
So we’re sharing it with you here and on The Breathe Institute’s channels.
When only one view is expressed, then we do not move forward as a society, and we do not collaborate and come together for the sake of the kids. It deepens the divide as is evident in our country at the moment in politics and many other issues. People can be mean and cold to those who don’t share their views. Attacks are made by both sides. Let’s look at the bigger issue here, and see how we can move forward together.
To learn more about tongue-ties, check out our multidisciplinary (and peer-reviewed) bestselling book on tongue-ties, available on Kindle, Paperback, and Hardcover on Amazon.com (LINK) and audiobook Audible.com (LINK). We also have several online courses and for providers, an Advanced Live Patient course.

Letter to the Editor:
We thank the authors for highlighting the importance of a multidisciplinary approach in the diagnosis, treatment, and follow-up care for tongue-tied babies and mothers.1 We applaud the movement towards collaborations with IBCLCs, SLPs, and bodyworkers. However, we have significant concerns about the methodology of the study which limits its generalizability.
This is a level five study based on subjective decision-making only without validated measures. The authors assert that the level of frenotomy is increasing, which is true but misses the point. Frenotomy rates are increasing perhaps because many of the presenting symptoms have only recently been linked to the condition. The article states there is a lack of evidence for frenotomy, when in fact there are several randomized controlled trials and cohort studies with validated measures showing that frenotomy significantly improves the quality of breastfeeding when other interventions have failed.2,3 It should be noted that ankyloglossia, untreated in infancy, may contribute to speech, solid feeding, and sleep quality issues; mouth breathing; and impaired growth and development of the jaws.4,5 Considering these possible long term effects, it is concerning that the article offers a very limited fourteen-day follow-up for the babies involved, with no recommendation of post-operative stretching exercises to prevent reattachment and reoccurrence of symptoms.3
Most concerning, the authors fail to emphasize the importance of continued post-decision follow-up for babies with exam findings of tongue-tie who were denied surgical treatment. Treating the apparent symptoms of a tongue restriction alone (e.g. acid reflux with medication) does not adequately address the underlying cause of the symptoms and may have negative long-term effects.5
Unfortunately, misinterpretations of this manuscript are being promulgated by the media as conclusive evidence that tongue-tie surgery is unnecessary for babies with tongue restriction. We hope this letter offers a more balanced perspective.
-Soroush Zaghi, MD; Chelsea Pinto, DDS; Richard Baxter, DMD, MS.
References:
- Caloway C, Hersh CJ, Baars R, Sally S, Diercks G, Hartnick CJ. Association of Feeding Evaluation With Frenotomy Rates in Infants With Breastfeeding Difficulties. JAMA Otolaryngol Head Neck Surg. July 2019. doi:10.1001/jamaoto.2019.1696
- Buryk M, Bloom D, Shope T. Efficacy of neonatal release of ankyloglossia: a randomized trial. Pediatrics. 2011;128(2):280-288.
- Ghaheri BA, Cole M, Mace JC. Revision Lingual Frenotomy Improves Patient-Reported Breastfeeding Outcomes: A Prospective Cohort Study. J Hum Lact. May 2018:890334418775624.
- Yoon AJ, Zaghi S, Ha S, Law CS, Guilleminault C, Liu SY. Ankyloglossia as a risk factor for maxillary hypoplasia and soft palate elongation: A functional – morphological study. Orthod Craniofac Res. 2017;20(4):237-244.
- Baxter R, Hughes L. Speech and Feeding Improvements in Children After Posterior Tongue-Tie Release: A Case Series. International Journal of Clinical Pediatrics. 2018;7(3):29-35.