These tongue-tie myths are repeated all too often. Medical professionals, dental professionals, therapists, friends, and family are prone to repeat these myths when they have not had up-to-date education on the topic. Educate yourself and others, or check out our longer articles on the subject, Part 1 and Part 2.
1. “A Clip or a Snip with Scissors Is Enough”
Often a snip or clip leaves thick tissue behind and will need a second proper release. The patient often sees some improvement, but the standard “clip” without post-op exercises is likely to be incomplete or grow back. A full release of restricted fascia will allow better function and symptom resolution. The laser allows complete visualization of the surgical area with typically no bleeding and ultimate precision, so we get all the tight tissue while protecting important structures under the tongue.
2. “The Tongue-Tie Will Stretch Out”
The tongue-tie is comprised of a thick webbing of fascia (mainly type 1 collagen fibers) that stretches less than 1%. If left untreated, it will persist into adulthood, and although some children can remarkably compensate with a tight tongue, no child should have to miss out on proper development and struggle with daily activities for a condition that is so easily treated.
3. “Tongue-Ties Rarely Cause Issues”
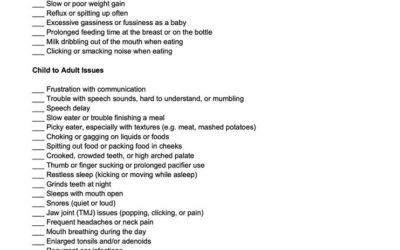
Breastfeeding, bottle-feeding, poor weight gain, reflux, colic, gassiness, speech delay, slow eating, choking and gagging, poor sleep quality, snoring, and teeth grinding are related to tongue ties and very often (84-89% in our study) see improvement once correctly released. Adults may struggle with headaches, neck pain, shoulder tension, and poor sleep or speech.
4. “Treating Tongue-Ties Is A Fad”
Tongue-ties have been written about for thousands of years, and until the 20th century were commonly released because it was clear that it impeded normal function. In the 1920s, treating tongue-ties fell out of favor. With the renewed emphasis on breastfeeding, we are now seeing increased diagnosis as well as treatment because, for decades, it has been virtually ignored, and many parents and professionals are not aware of the issues it may cause. It also seems to be increasing in incidence due to unknown factors, just as autism is increasing in awareness and incidence. Treating autism is not a fad, and neither is treating tongue-ties.
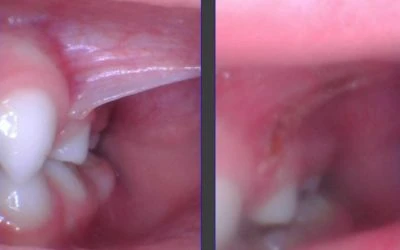
5. “Posterior Tongue-Tie Doesn’t Exist”
A posterior tongue-tie is simply a symptomatic tongue restriction. Restricted fascia or webbing under the tongue is sometimes clearly visible, and other times is not easily seen. The baby or child who has no obvious string but has all the symptoms of a tongue-tie often has a posterior tongue-tie. It is seen by elevating the tongue with two index fingers from behind, and the tight webbing of fascia will be visible. When released, they see symptom improvement no different from a to-the-tip tie because now the posterior aspect of the tongue can elevate better allowing for improved swallowing, speech, and sleep because the tongue resting posture changes and no longer falls into the airway.
6. “They Will Just Laser Everyone”
We ensure that each patient has a thorough history, typically spending 30 minutes or more talking with the family before examining the patient. We don’t want to overtreat or undertreat anyone. We examine with magnification and a headlamp, and from behind so we can accurately assess restrictions. We have a lengthy discussion with parents to not mislead or overpromise results and to set realistic expectations for the procedure. The procedure is quick (around 15 seconds) and is not any more traumatizing than a routine vaccine, and much faster than circumcision. The CO2 laser is ultra-precise removing the width of a human hair at a time so it’s easily controlled and safer than scissors, scalpel, diode laser, or cautery which can cause iatrogenic damage if the patient were to move. We only perform the procedure when it is significantly affecting the quality of life, and we turn patients away who do not have significant issues and counsel them not to do one or both areas (lip or tongue) as determined by symptoms and the examination.
7. “Just Give It Time”
Many issues in pediatrics will improve with time. Telling a mother who is having toe-curling pain and struggling to nurse to just “give it time” is unhelpful. Bottle-feeding babies who still struggle with excessive gas, slow feeding, milk leaking out of the mouth, and reflux often have a tongue-tie and will continue to struggle. Children with solid feeding or speech issues very often have a tie. Traditional speech therapy does not assess for ties, and will try to have the child compensate to achieve normal-sounding speech, but incorrect tongue placement to make sounds can lead to dental development issues and more effort when speaking. It’s wise to remove the physical impediment if it is easily completed with little trauma and great potential reward. Inaction can often be more harmful than action.
8. “They Must Be Doing It For The Money”
Trust me, dentistry is more productive monetarily than treating tongue-ties! Why do we do it then? It’s very rewarding. Parents are so thankful that their baby can now eat without getting frustrated, and mom has less pain. Kids who are speech delayed often start talking more and more clearly. Kids with poor sleep finally sleep deeply and even have better behavior. Kids with poor feeding can finally go out to eat at a restaurant as a family because it’s not a big struggle to feed the child. In our recent prospective IRB-approved study, at one month after the procedure, 89% of kids with speech issues had improved speech, 84% of those with feeding issues had improved feeding, and 84% with sleep trouble had improved sleep.