The process of feeding your infant should be a peaceful one, and it should not become a struggle between you and your baby during every feeding session. Moms experience exhaustion and physical discomfort while their baby goes through yet another difficult period, and looks at you with longing eyes and seemingly asks you to “figure out what is wrong with my feeding, mom!” Sadly, well-meaning family members or healthcare providers say the baby is “fine” and will gain weight ok, so just wait it out, maybe 4–6 months, and it will get better. But in your gut, you know something is off.
The solution to many feeding problems in infants can be found in a baby’s upper lip-tie or tongue-tie (and sometimes cheek-ties, aka buccal-ties) since the baby struggles to latch or transfer efficiently, and has a poor seal, so swallows too much air.
The medical community fails to recognize lip-tie in newborns as a condition that affects newborns more than any other common medical condition. The medical community has studied tongue-tie extensively, yet families dealing with lip-ties continue to experience frustration because they cannot find answers to their problems. Lip-tie and tongue-tie often go together in babies. Many babies have what appears to be a lip-tie, so it’s helpful to know the common symptoms and when treatment is needed.
This guide reveals what to do about an upper lip-tie in newborns that most parents and even some providers overlook.
What is a lip tie in a newborn?
Our discussion of upper lip tie in a newborn begins with its most fundamental definition.
Every baby has a frenulum or frenum – a thin tissue connecting the upper lip to the gum. A lip tie in newborns occurs when the tissue is abnormally thick, tight, or short, preventing the upper lip from moving freely. Some are thin and tight, others are thick and corded. They come in all shapes and sizes.
Why does that matter?
The upper lip needs to extend outward during feeding because this action creates a strong seal that allows proper breastfeeding and bottle-feeding. When a lip-tie in newborns prevents this, feeding becomes inefficient, painful, and exhausting – for both baby and parent.
The medical and dental system (Kotlow classification) uses four classes to define lip-ties, beginning with Class I (minor) and progressing to Class IV (which extends into the hard palate). The need for treatment arises from more factors than those captured by the existing classification system. Appearance shows less importance than functional capabilities. A thin upper lip tie in a newborn who can’t feed effectively needs attention just as urgently as one with a severe classification.
Upper Lip Tie vs Normal: Spotting the Difference
Parents can identify early signs of problems by understanding what an upper lip-tie is and what normal lip movement looks like.
A normal frenulum appears as a thin elastic band that extends above the gum line. The lip lifts freely and flanges outward without resistance during feeding. There is no pain or distress to the baby when flipping the lip outward.
Newborn babies show different lip-tie symptoms when they have an upper lip tie. The tissue appears thick and tight. The attachment point can be located at two positions: low on the gum ridge or beyond it. The lip movement of your baby will show two signs: the lip will resist movement and become pale at the attachment point. There will be a crease on the outside of the lip as well. The lip will also curl under instead of flipping out like “fish lips.”
Many parents fail to notice this visual sign, which shows when their baby cries, which could cause their upper lip tie in the newborn to form a notch in the center or the tissue to blanch (turn white). The restricted frenulum pulls the lip downward from its normal position. The behavior is not only a cute habit but also a medical condition that needs further study.
Hidden Symptoms of Lip Tie in Newborn Babies
Most parents recognize the common signs of a lip tie in newborn babies: a shallow latch, clicking sounds, and nipple pain. But several critical lip tie in newborns symptoms fly completely under the radar:
Reflux That Won’t Quit
An upper lip tie in a newborn baby prevents a proper seal, causing them to swallow excessive air during every feeding. The result? Spitting up, back arching, and irritability that perfectly mimic acid reflux or colic. Parents cycle through medications and formula changes without improvement because the root cause isn’t acid. It’s aerophagia from a poor oral seal.
Newborns typically develop sucking blisters as a normal occurrence. The upper lip develops recurrent blisters or calluses because the lip struggles to move when breastfeeding or bottle-feeding. This is due to overuse of the lip and sometimes insufficient tongue mobility (maybe a tongue-tie, too – they often go together).
Feeding Exhaustion Disguised as Sleepiness
A baby who drifts off to sleep after five minutes of feeding isn’t necessarily satisfied. Babies with lip tie baby symptoms burn tremendous energy trying to extract milk. The process repeats itself because they sleep for short periods before waking up hungry, which creates an exhausting cycle that appears to be normal or just “cluster feeding.” Again, a lip or tongue-tie can lead to these issues, so it’s best to get checked for both.
Bottle-Feeding Struggles
Upper lip tie in newborns affects both breastfeeding and bottle-feeding. The combination of milk leakage (messy eater), reflux, colic, nose congestion, difficulty with nipple preference, and excessive gas (burping or tooting) are common symptoms that lip tie in babies can lead to, and often bottle-feeding families fail to recognize.
The Tucked Upper Lip During Feeds
Parents need to observe the position of the upper lip because lip ties in babies are common and can affect feeding. The lip can be in two possible positions: flanged outward like a fish lip, or curled inward and tucked tight. A lip that won’t flange is one of the most reliable – and most overlooked – functional signs of restriction. If you try to flip it out, the baby often cries or is in pain, just like if you took my arm behind my back farther than it wanted to go, past its normal range of motion.
Next Steps That You Need To Take
Families experiencing these symptoms should see a provider with expertise in tethered oral tissues, including pediatricians, IBCLCs, some pediatric dentists, and pediatric ENTs. You have to ensure that the provider is up to date on the latest diagnostic and treatment protocols for upper lip tie, as this information is not taught in medical, dental, or even lactation programs. Sadly, many providers will dismiss the mother’s concerns or say the child will be fine and “fall and rip the lip tie” or will “grow out of it,” which doesn’t happen for years. This offers no help to the nursing or bottle-feeding baby, and instead, problems persist. The evaluation of oral function should include all aspects of oral function because lip and tongue ties usually coexist. Using a symptom sheet is an easy way to check for tongue and lip-tie symptoms; if there are more than a few items on this sheet affecting your baby, it’s worth getting an evaluation.
Most providers are not looking through this “lens” of lip-tie, so they see reflux, colic, gas, spitting up, nasal congestion, and trouble latching as all independent issues. So instead, they give acid reflux medication, gripe water, gas drops, switch to a bottle, nasal saline, and a nipple shield – a bunch of band-aids instead of addressing the root cause! This root cause is often a lip or tongue-tie.
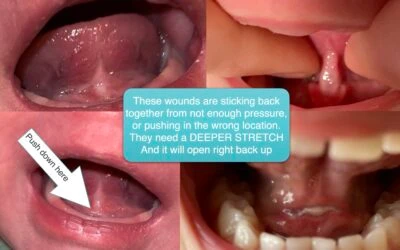
An upper lip tie in a newborn may require a frenectomy, which is the removal of the frenum, because other methods, which include latch adjustments, possibly medications, or other compensations, have failed. The surgery can be performed with scissors (need more than just a clip or a snip), which can be bloody, or we use a state-of-the-art CO2 laser, and it takes around 10-15 seconds with minimal bleeding. A lip-tie release or frenectomy removes all the restricted tissue, which enables most infants to breastfeed right after the procedure with better results. Often, a lip and tongue-tie go together, so both are treated simultaneously, at around 15 seconds for the lip and 5 to 10 seconds for the tongue. We do not sedate or put the babies to sleep, as this introduces unnecessary risk, and the baby is back in the mother’s arms in around 4 minutes and can nurse right away. Stretches are needed after the procedure to maintain the new mobility and ensure it does not reattach or stick back together.
Trust Your Own Judgment / Mother’s Instinct
A lip tie in newborns is a real issue and is treatable, with positive symptom improvement when diagnosed and treated promptly and properly. If feeding feels impossibly hard despite your best efforts, understand that the issue is not you or your fault! The issue very well may be structural and highly treatable. If there are no symptoms, and the baby is feeding fine, then there is likely nothing to do, and you probably wouldn’t be reading this article! But if there are symptoms, seek help from a provider who will assess the symptoms on the sheet and will take your concerns seriously instead of prescribing band-aids.
Trust your instincts. Seek helping hands. Both you and your baby are entitled to peaceful feeding and a proper mother-infant bonding experience. Dr. Baxter treats tongue-tied and lip-tied patients from around the country and across the world. In just a single visit, we can assess, treat, and see results in most cases. We would be honored to help your family. Just give us a call at 205-419-4333 or send us a message to set up a consultation with Dr. Baxter or Dr. Trego.
FAQs
Q1. What are the common symptoms of a lip tie in newborns?
Common lip tie in newborns symptoms include difficulty latching, clicking sounds during feeding, nipple pain, gas, reflux, colic, nose congestion, frustration at the breast, and milk leaking from the baby’s mouth.
Q2. How can parents identify an upper lip tie in newborns?
An upper lip tie in a newborn may appear as thick or thin tissue attaching the lip tightly to the gum, preventing the lip from flaring or flanging outward during feeding.
Q3. Can a lip tie in newborn babies affect bottle feeding?
Yes, lip tie in babies can make bottle-feeding difficult by causing poor seal, milk leakage, reflux, colic, gas, and congestion from excessive air swallowing.
Q4. Does every upper lip tie in babies require treatment?
Not always. Treatment is recommended only if the upper lip tie in babies causes feeding problems, a poor latch, or some other symptom from the sheet.
Q5. Who should diagnose a lip tie in newborns?
A lip tie in newborns should be evaluated by professionals such as pediatricians, IBCLCs, pediatric dentists, or pediatric ENT specialists. We would be happy to help your family. Just give us a call at 205-419-4333 or send us a message.